A therapy progress note updates a prescribing physician on their patient’s current status towards their rehab goals. This kind of note can also take the place of a daily note, since it follows the standard SOAP formula for daily documentation.
In keeping with SOAP, a progress note typically includes the following items (which also outline our table of contents for this article):
Table of Contents of Article:
- Subjective and Summary of Treatments Provided
- Objective: ROM, strength, special tests
- Assessment and Goal Status
- Plan and Recommendation
- Physical Therapy Progress Note Examples
When writing a progress note, understand that the physician may have less than a minute to review your notes. Be clear and to the point as you highlight key findings in your assessment.
Sometimes it’s helpful to put a star or asterisk next to an important finding if you feel that it might go unnoticed in the rest of the progress note.
Writing a Progress Note By Section
Let’s take a look at important items to include within a given physical therapy progress note.
Subjective
Give a brief statement on how the patient feels they have been progressing since starting PT (their subjective experience of therapy).
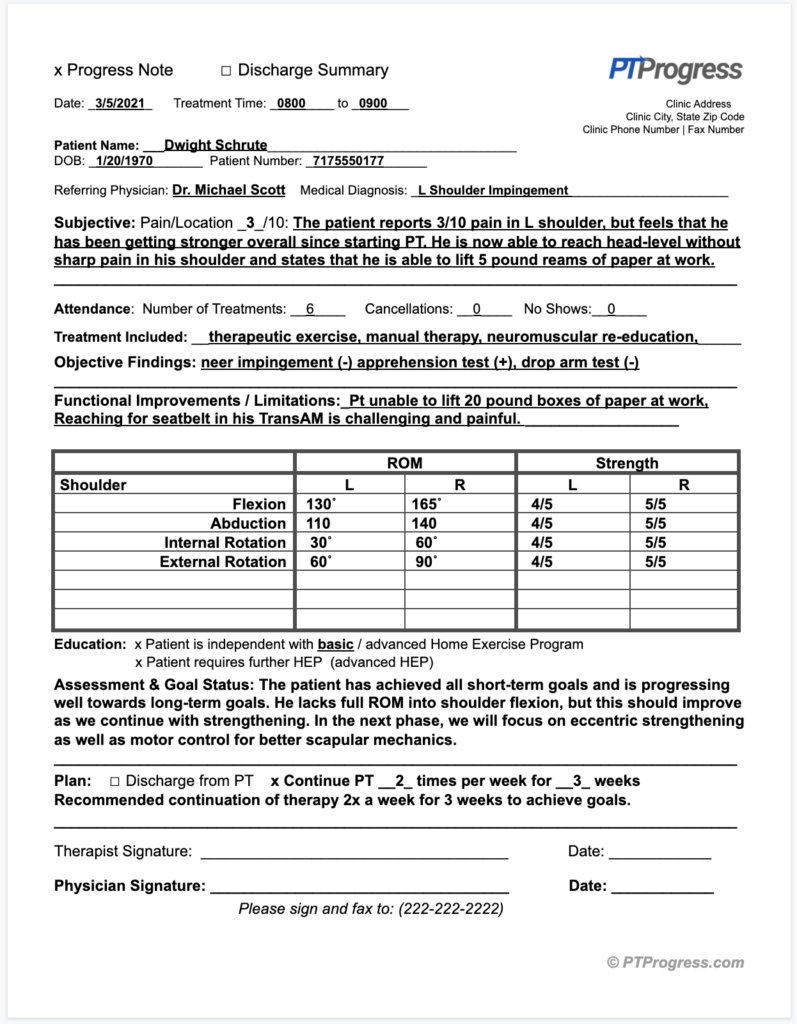
The patient reports 3/10 pain in his shoulder, but feels that he has been getting stronger overall since starting PT. He is now able to reach head-level without sharp pain in his shoulder.
Summary of Treatment Provided
A progress note also reports a summary of provided treatments and the number of completed visits. This gives the physician an idea of how many visits/cancellations their patient has had as well as the types of treatments you’ve provided.
Your treatments may include the following: therapeutic exercise, manual therapy, neuromuscular re-education, balance/gait training, iASTM, E-Stim, Ultrasound, etc. I’ve included a line for this summary in my sample progress note template.
Objective: ROM, Strength, Special Tests
It’s important to include relevant special tests in your Objective report – keyword, “relevant.” Don’t include every possible special test; that would make it difficult for the physician to locate pertinent findings. Include only the most relevant tests and indicate whether it is a positive (+) or negative (-) finding.
For example: ex. Neer Impingement (-), Apprehension test (-), Drop arm (+), etc.
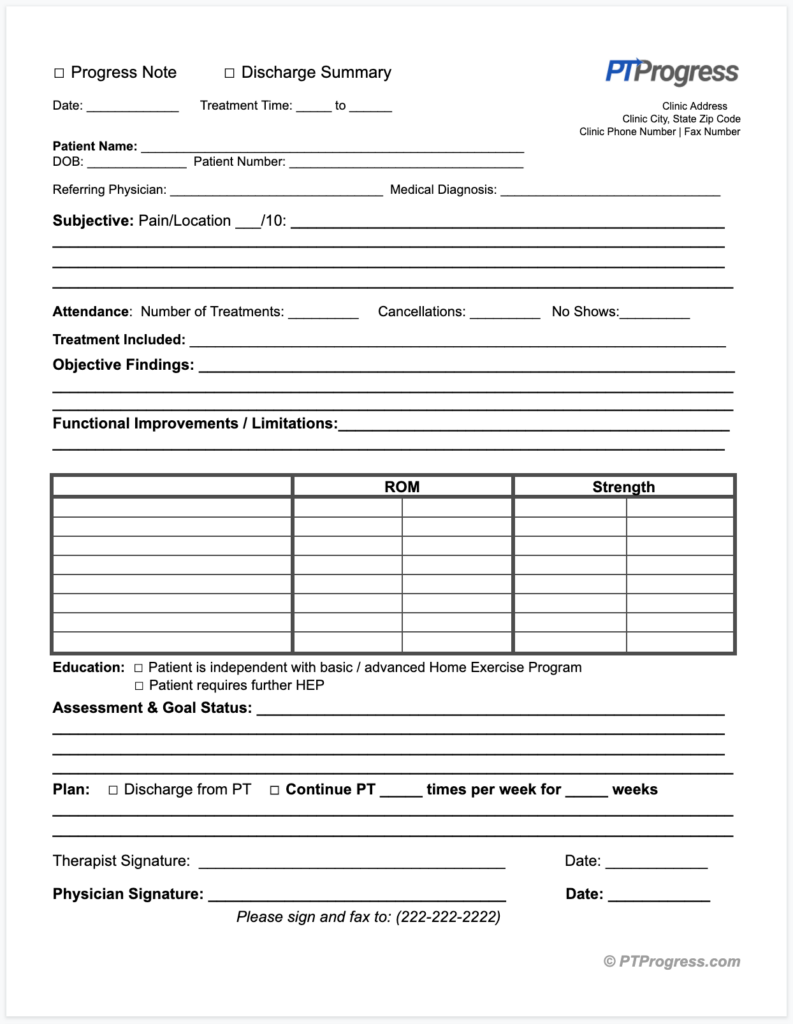
Including previous ROM is a quick way to document progression or regression. It’s also helpful to present your data in a grid format, especially for ROM and strength measurements. You’ll notice my progress note template includes this format.
Assessment and Goal Status
In this section of your progress note, the physician will want to read your overall thoughts on the patient’s progress towards their goals and how you expect to advance their treatment.
Using a couple lines of space, you may write something like the following:
The patient has achieved all short-term goals and is progressing well towards long-term goals. He lacks full ROM into shoulder flexion, but this should improve as we continue with strengthening. In the next phase, we will focus on eccentric strengthening as well as motor control for better scapular mechanics. Recommended continuation of therapy 2x a week for 3 weeks to achieve goals.
Plan
Some therapists lump together the Assessment and Plan sections of a progress note. However, you’ll notice in my sample progress note (downloadable here), I’ve included a separate line for the Plan.
Here’s a brief line you might include in the Plan section:
Will continue to progress with strengthening of the shoulder, including stabilization techniques and PNF manual resistance. Recommended to continue 2x a week for 3 weeks.
Physical Therapy Progress Note Examples
You can download – for free! – my sample progress note for therapists and learn how to write a progress note quickly and efficiently. Whether you are a cash-pay physical therapist, school-based PT or OT, or an outpatient therapist, this progress note outline will save you a lot of time.
You became a physical therapist to help people move better, but part of your job involves writing documentation, such as daily notes or therapy progress notes. If you’re wondering how to write a progress note or need some templates to get you started, I have just the resources to help you out!
If you are interested in saving even more time with your documentation, check out my Therapy Documentation Templates. These smart, PT “cheat sheets” provide over 60 assessment examples to help save you 30 minutes each day on your documentation.